
In this section, we define and discuss the concept of motor control and motor learning to improve performance.
Intervention strategies that can be used to promote skilled performance and motor learning are also discussed.
- Motor control is a complex process involving the coordinated contraction of muscles due to the transmission of impulses sent from the motor cortex to it’s motor units. It is “the process of initiating, directing, and grading purposeful voluntary movement” (physiopedia)
- It is a top-down process of the nervous system that occurs before the actual movement is performed (planning –> programming –> execution), that appropriately adjusts for force, tone and timing.
- During the intended movement goal, the nervous system continues to assess it’s performance and adjusts force, timing and tone accordingly with sensory information from proprioceptors, visual and vestibular systems
- This information that is obtained can be stored from future performance of the same task. If this is then repeated, a new skill can be learnt. See ‘What is motor learning” below.
- The aim is to reduce the cognitive demand during a skill or task i.e. learning to drive and talk at the same time.
Motor Control Theories include production of reflexive, automatic, adaptive, and voluntary movements and the performance of efficient, coordinated, goal-directed movement patterns which involve multiple body systems (input, output, and central processing) and multiple levels within the nervous system.
As therapists we can change the environment, or the task in such a way as to enable our patients to achieve their goals.
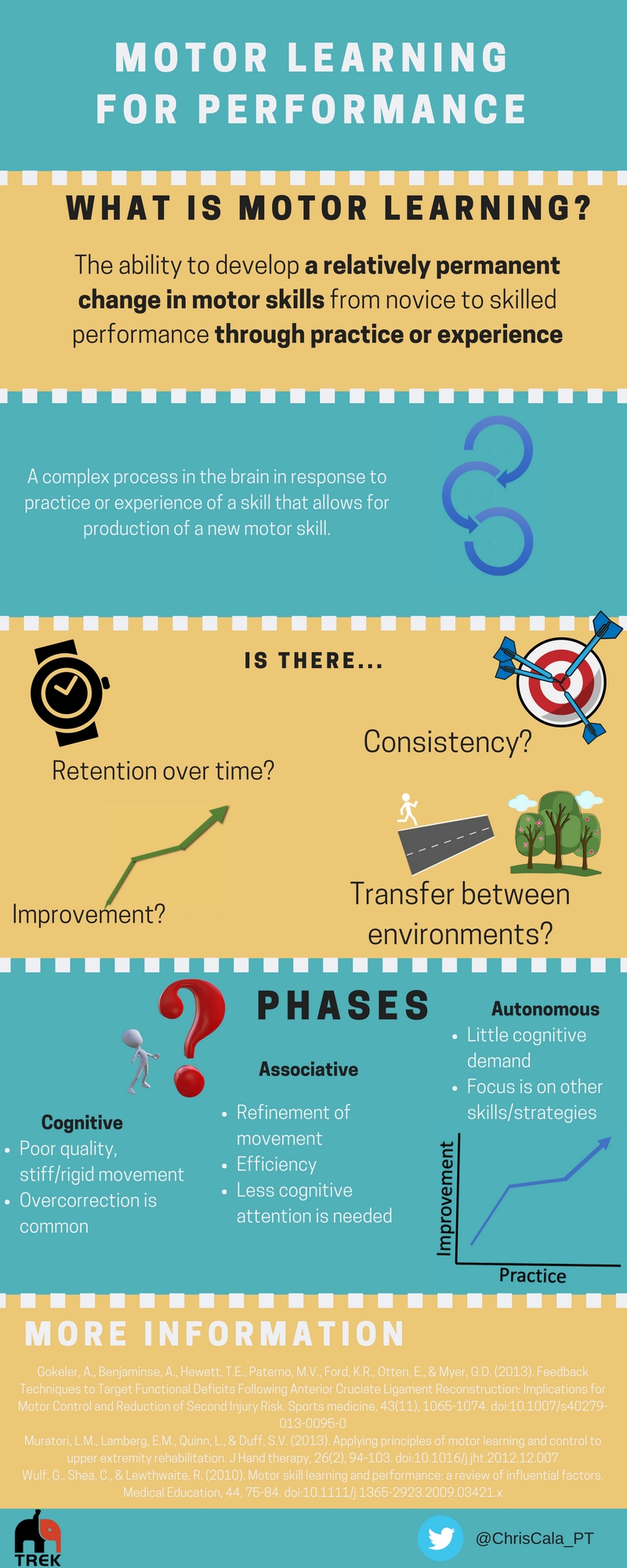
- The ability to develop a relatively permanent change in motor skills from novice to skilled performance through practice or experience by engaging in activities that are currently beyond an individuals capabilities (Muratori, Lamberg, Quinn, & Duff, 2013; Gokeler et al, 2013).
- It is when complex processes in the brain occur in response to practice or experience of a skill resulting in changes in the central nervous system that allow for production of a new motor skill.
To determine the success of motor learning and skilled performance the following concepts are used:
- Improvement – measuring the skill i.e. archery score, more accurately hitting a target. There should be a decrease in errors.
- Consistency – the individual is able to reliably produce the result
- Retention – Retention tests are used following a delay in practice to determine if permanent learning has occurred.
- Transfer – The ability to perform a similar movement, within a different context in which it was initially learnt is tested (transfer) i.e. changing the amount of force or surface, location etc (Muratori, Lamberg, Quinn & Duff, 2013).
During rehabilitation, progressing an exercise subsequently increases the amount of information to be processed. If the progression is added too quickly, the ability to understand the information may not have concurrently increased (Guadagnoli and Lee, 2004).
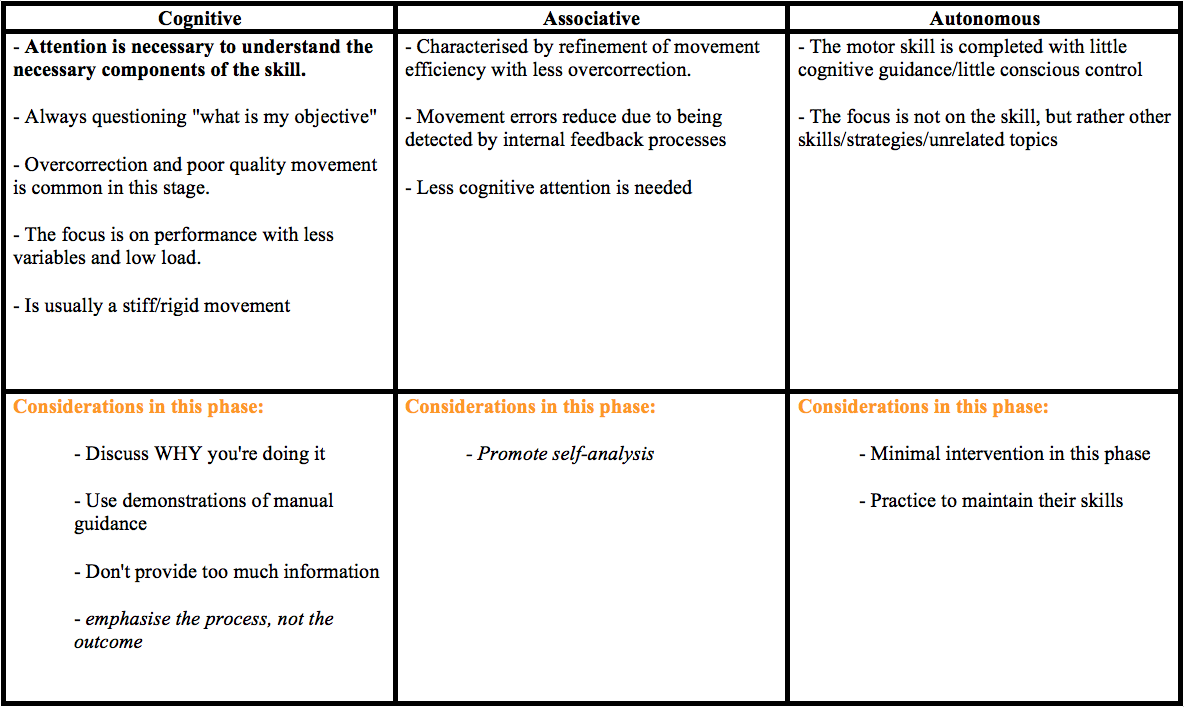
Motor learning typically involves 3 phases (Fitts, 1976);
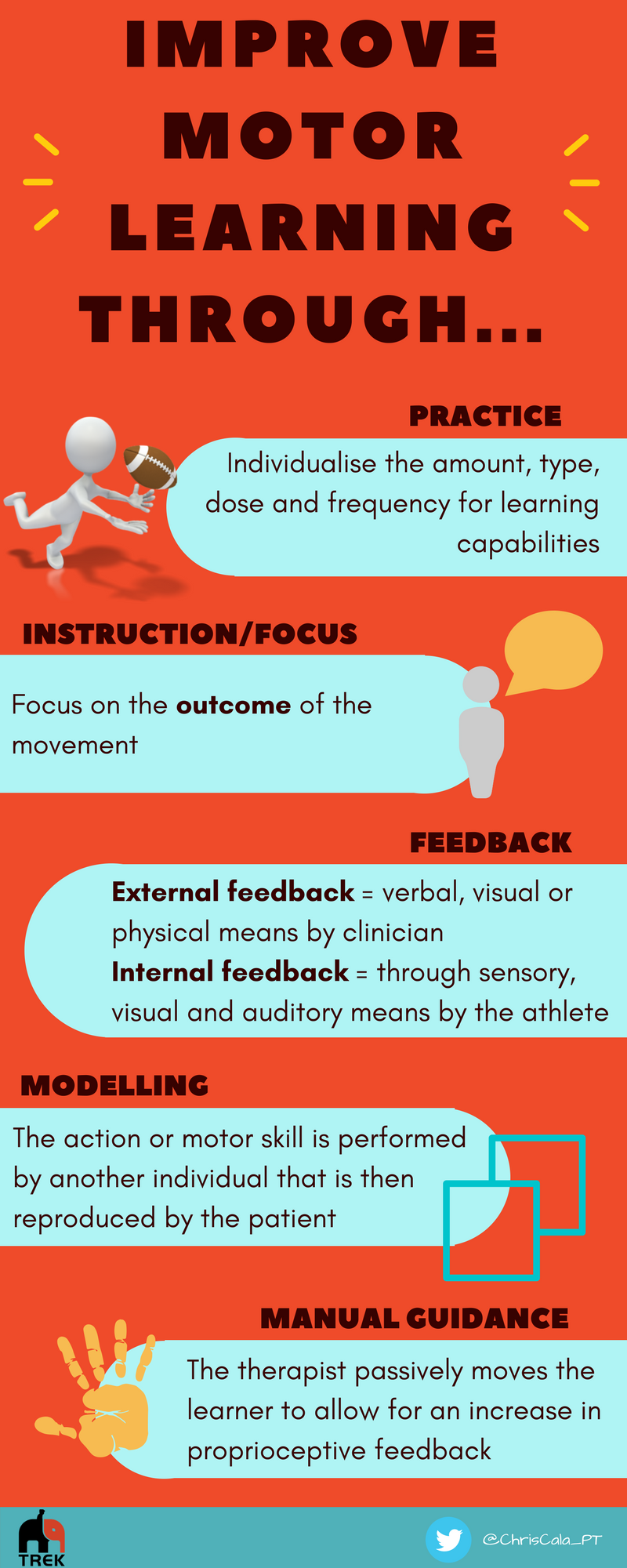
- Practice; An increased amount of practice is related to improved capabilities; however, the process of optimal learning is not clear-cut so the amount, type, dose and frequency must be individualised depending on learning capabilities
– Part-practice versus whole practice
– Mental practice
– Specificity of practice
- Instruction/focus;
– An external focus of attention should be used when providing instructions, with an emphasis on the outcome of the movement compared with instruction to direct attention to their own movement i.e. using “imagine kicking a ball” instead of “extend your knee more” when improving knee extension during stance following ACLR
– Using an external focus of attention allows the process of learning to happen more quickly, and can result in better performance by allowing the patient to develop their own strategies for movement (Gokeler et. al. 2013).
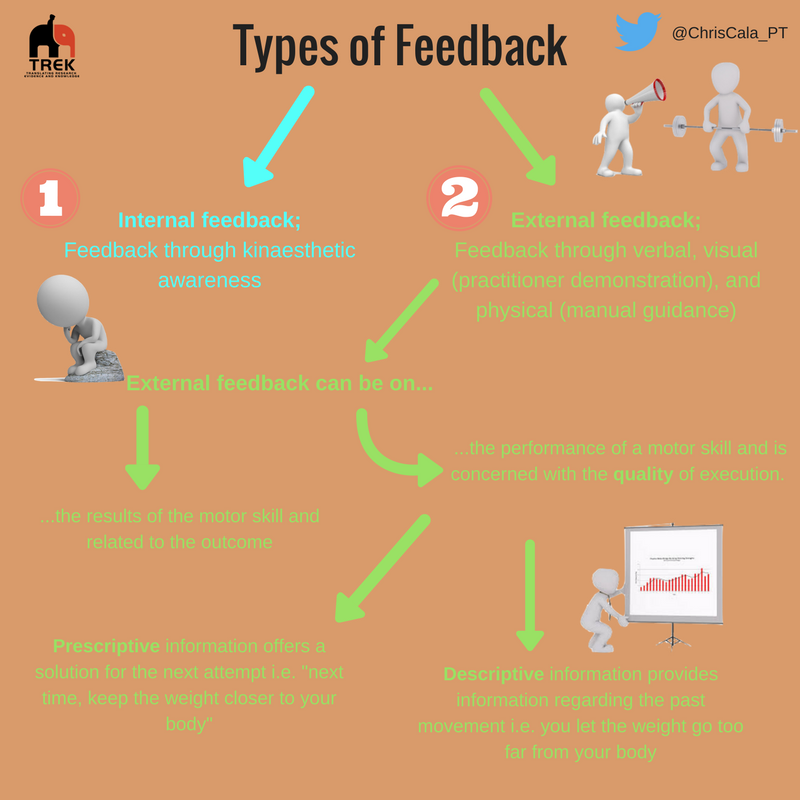
- Feedback; The frequency of feedback provided by the clinician can be during, or after the task is completed
– If feedback is repeatedly provided throughout a movement, it may hinder the ability of the learner to retain and successfully transfer the skill as they become passive participants whom reliant on feedback (Winstein, Pohl, Lewthwaite, 1994)
– The amount of feedback should be reduced as the learner progresses through their rehabilitation by providing intermittent summaries of performance, gradually reducing feedback over time, only provide feedback if large errors occur or allow the learner to guide feedback
– Internal feedback is providing information about the movement through sensory, visual and auditory means (Muratori et. al. 2013).
– Less feedback is usually best (Muratori, Lamberg, Quinn, & Duff, 2013).
![]()

- Modelling; the process by which the action or motor skill is performed by another individual that is then reproduced by the patient
– This can be beneficial due to social interaction, competition or increased motivation.
- Manual guidance; the therapist passively moves the learner to allow for an increase in proprioceptive feedback
The clinician should provide a higher amount of feedback when initial learning is occurring, and gradually decrease the frequency as the patient becomes more proficient, especially with complex tasks. This feedback can be through verbal, visual, or physical means and be directed to the patients learning ability and cognition. When providing instructions for motor skill learning, aim to utilise cues that direct the attention to the effect of the movement versus describing how to move individual body parts – this will improve learning and allow the patient to develop their own solutions to problems.
- Motor Control theories. Presentation by Dr. Duane “Spike” Millslagle, Associate Professor Exercise Science, University of Minnesota
- iKnowlege – Contemporary issues and theories of motor control, motor learning, and neuroplasticity
- Motor control theories and their applications
- Essential Concepts of Motor Control & Learning. Presentation by DM McKeough.
Supporting Texts/Articles/Medias
Medical Dictionary for the Health Professions and Nursing. (2012). Retrieved March 11 2016 from http://medical-dictionary.thefreedictionary.com/motor+learning